



.png)
.png)
The Kitchen We Didn’t Design: Lived Experience as Advocacy

March 25, 2026

Over ten million senior citizens aged 65 and older live with a cognitive impairment, seven million of whom have Alzheimer's disease. By 2033, the US senior population is forecasted to grow by 45%, and so too will the number of people with Alzheimer’s and other forms of dementia. In an effort to address the needs of this growing population, in 2017 the Centers for Medicare & Medicaid Services (CMS) started covering cognitive assessments as part of the Medicare Annual Wellness Visit—a preventive care visit free to Medicare beneficiaries enrolled in Part B.
To date, it appears that, regrettably, few patients and providers are benefiting from this tool. In a recent report entitled “Medicare Cognitive Assessments,” Congress’s Government Accountability Office (GAO) shared that only 2.4% of traditional Medicare recipients with an Alzheimer's diagnosis have received a cognitive assessment. This is due to a myriad of factors, including strained PCP schedules, insufficient training, and lack of patient proximity to physicians able to administer the assessment.
Synapticure was founded with the mission of democratizing specialized care for all and, as such, we are deeply committed to supporting PCPs and neurologists in caring for patients living with dementia. Our team is licensed to care for patients in all fifty states, and our telehealth platform enables us to see patients in all geographic regions, including those in rural and underserved communities. We are able to help care for patients living with dementia at any stage, from pre-diagnosis to hospice, and look forward to helping expand the use of Medicare’s cognitive assessment as an integral part of dementia care.
Medicare’s Annual Wellness Visit (“AWV”) now provides coverage for providers to conduct a 60-minute examination to assess if any cognitive impairments exist. Under Medicare guidelines, providers can perform cognitive assessments on any patients “showing signs of, or already diagnosed with, a cognitive impairment.” For many reasons, time is of the essence with a cognitive assessment. Per the GAO Report:
“Diagnosing cognitive impairment and developing a plan of care may help manage symptoms, improve quality of life, and give beneficiaries the chance to take part in care decisions before their impairment becomes severe.”
Signs of cognitive impairment include trouble remembering or learning new things; difficulty concentrating; problems managing finances or making decisions about your everyday life; or changes in mood and personality.
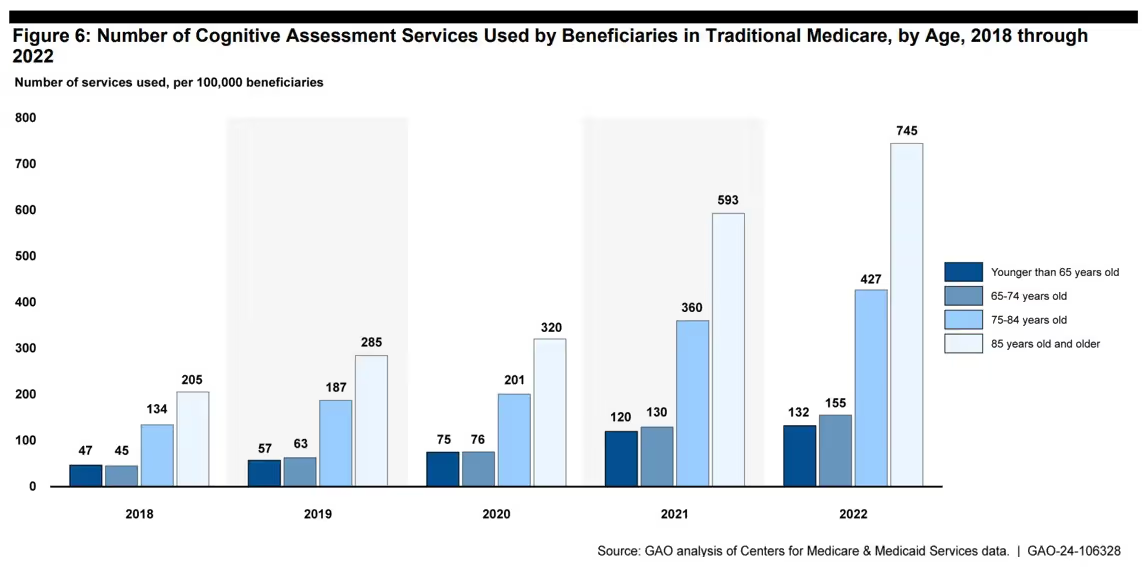
The GAO examined data from traditional Medicare recipients from 2018-2022 and its report provided information about: (1) utilization of the cognitive assessment service and (2) challenges providers face in delivering cognitive assessments. In the last three years, utilization of this CMS-covered service has tripled, but with only 2.4% utilization, there is still much opportunity to increase early identification of cognitive impairment. As you can see from the graphic below, the age group with the highest participation are those 85+ years old. However, there are likely many missed opportunities to identify mild cognitive impairment and to implement a care plan for those within much younger senior populations.
Women are 2x more likely to be diagnosed with Alzheimer’s than men. Thus, as expected, female Medicare beneficiaries used more cognitive assessment services than male beneficiaries. By 2022, cognitive assessments were performed on female beneficiaries at a rate of 325 per 100,000 versus 242 per 100,000 male beneficiaries. Across all age groups, women used the cognitive assessment service more often than men.
The 2021 American Community Survey estimated that 59.9 million Americans are over the age of 65. According to the US Census, more than 1 in 5 of those older Americans live in rural areas, many concentrated in states where more than half of their older populations are in rural areas.
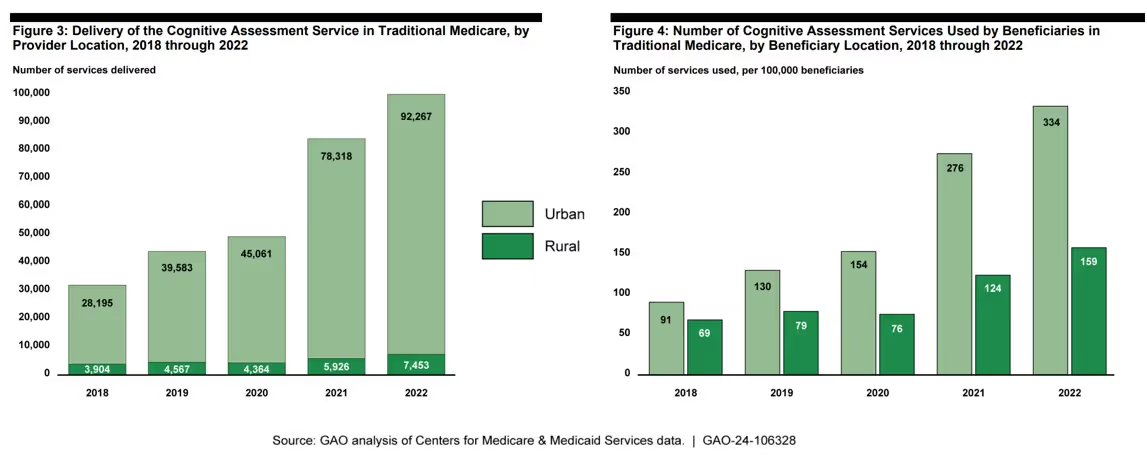
While there are significant opportunities to improve the number of seniors getting cognitive assessments, this need is more profound in rural communities where there are often “care deserts.” As demonstrated in the GAO’s graphics below, urban beneficiaries in traditional Medicare used the cognitive assessment service about twice as often as rural beneficiaries in 2022—likely due, in substantial part, to lack of access to rural physicians with expertise in CMS’ cognitive assessments.
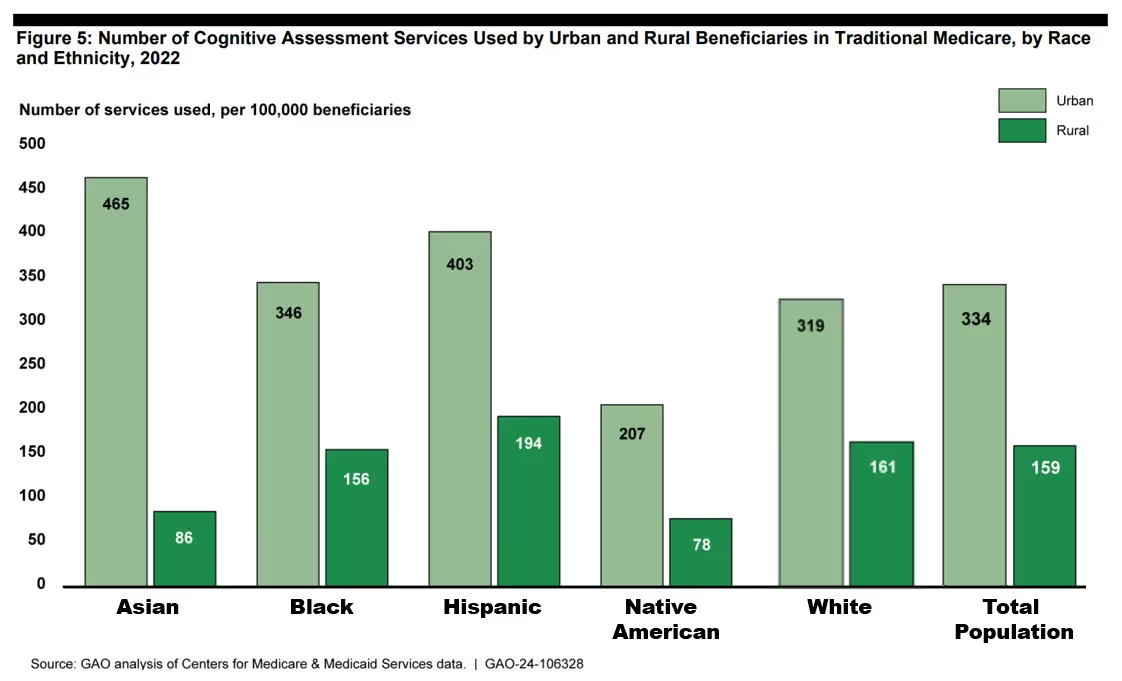
The country’s 12 million Black and 19 million Hispanic Americans have a 2x and 1.5x higher risk of developing dementia, respectively. In the GAO report, they found that Black and Hispanic Americans are receiving cognitive assessments at similar or higher rates, per 100,000, as White Americans.
However, these assessments are not occurring on a timely basis to optimize care plans. As we reported in our blog:
“A higher proportion of Black and Hispanic Americans experience a diagnostic delay from symptom onset. The average delay for White Americans is 31 months, whereas it is 35 months for Black Americans and 44 months for Hispanic Americans. And according to this 2022 study, Black and Hispanic Americans are typically diagnosed in the later stages of dementia when they are more impaired, and need more medical care.”
Several barriers contribute to the delay and prevent people of color from accessing the highest quality care, including healthcare prejudice and disparities, lack of culturally competent care, and systemic racism. However, Hispanic and African Americans are forecasted to see the largest increases in ADRD in the future. By 2060, Alzheimer’s disease is predicted to afflict an estimated 14 million people, with Black Americans experiencing a 4x increase and Hispanic Americans experiencing a 7x increase. Thus, this magnifies both the importance and the need for a prompt diagnosis, which in turn, illustrates the importance of Medicare's cognitive assessment program.
The GAO report only focuses on Medicare Part B beneficiaries, but a 2020 study by USC’s School of Gerontology compared the traditional Medicare population with Medicare Advantage beneficiaries. Among its findings, approximately one-half of all Medicare Advantage beneficiaries reported having an AWV, but only about a quarter reported receiving a structured cognitive assessment at that visit, even though detection of cognitive impairment is a required component of the AWV.
Compared to traditional Medicare beneficiaries, Medicare Advantage beneficiaries were:
According to CMS, the cognitive assessment includes a detailed history and patient exam, including input from an independent historian such as family, friend or guardian who can provide the patient’s reliable medical history. The practitioner will perform the following elements during the cognitive assessment:
In the GAO report, both patients and providers described barriers to the performance of cognitive assessments. Patients and beneficiary advocacy groups spoke of the stigma associated with a cognitive diagnosis, but also a lack of awareness that the service was available, and misconceptions that cognitive issues were the inevitable result of aging.
But providers like primary care physicians (PCPs) described different challenges.
Although CMS adopted the cognitive assessment service to give PCPs more options for delivering cognitive care services, stakeholder groups also reported that PCPs have limited training on how to conduct cognitive assessments or develop care plans, with one group noting that this limited training may lead to “missed observations about a patient’s condition” during a cognitive assessment. As such, numerous PCPs suggested that specialists, like neurologists and geriatricians, are “better suited to deliver the cognitive assessment service.”
In our recent blog entitled “Rising Epidemic of Alzheimer's Disease & Risk Factors for Aging Americans,” we discussed similar concerns expressed by PCPs in a survey by the Alzheimer’s Association:
“More than half of PCPs reported that there were not enough specialists in their own geographic area to meet patient demand, which resulted in 8 in 10 PCPs handling the burden of dementia diagnosis and care. This creates an incongruity in patient care as nearly 1 in 4 PCPs had no residency training in dementia diagnosis and care. Even among those who did receive some training, 2 in 3 said the amount was ‘very little’.”
The provider deficit is not just among PCPs, but includes neurologists as well. In a 2020 study published in Neurology entitled “Geographic Variation in Neurologist Density and Neurologic Care in the US,” the authors raised concerns about this discrepancy. It found that people in rural communities with dementia are less likely to see a neurologist, with one of the study’s authors warning:
“Our research found that some areas of the country have up to 4 times as many neurologists as the lowest served areas, and these differences mean that some people do not have access to neurologists who are specially trained in treating brain diseases.”
According to the GAO report, of the traditional Medicare beneficiaries who received the cognitive assessment service in 2022, 22% were diagnosed with mild cognitive impairment, 12% were diagnosed with Alzheimer’s disease (including both early and late onset), and another 12% were diagnosed with unspecified dementia without behavioral disturbances. Vascular dementia, unspecified dementia with behavioral disturbances, and age-related cognitive decline all comprised 2% each. However, many other diagnoses resulted from the Medicare Cognitive Assessment program.
These CMS Cognitive Assessments are just the first step in getting proper care for people with Alzheimer's disease and other forms of dementia. These tests typically will only identify people who are experiencing a fair degree of cognitive decline and are often inadequate to identify those in very early stages of cognitive decline. Furthermore, these tests are seldom capable of diagnosing the cause of the cognitive decline – unless performed by a specialist. Thus, if you suspect someone is experiencing meaningful cognitive changes, we suggest patients talk with their PCP about whether a referral to a cognitive neurologist or neuropsychologist is appropriate.
Commenting on the lack of neurologists in underserved communities across the US, the former President of the American Academy of Neurology, James Stevens, MD affirmed that: "one way to give people more access to neurologic care is with telemedicine.”
The National Institute on Aging, too, is supportive of using telehealth to address gaps in dementia resources and care:
“Telehealth interventions offer a method of delivering dementia care that may be easier for people with dementia and their care providers who find it difficult to leave their home. With telehealth, health care providers can meet people where they are in their homes.”
Synapticure’s telehealth model can help address this incongruity in dementia care as our specialty neurology practice includes neurologists licensed in all 50 states, including cognitive neurologists and neuropsychologists who have spent their careers caring for people with Alzheimer’s disease and other forms of related dementia.
At Synapticure, we would be honored to help you, your loved ones or your patients who are dealing with dementia or anyone wanting to get a cognitive assessment as outlined by Medicare’s Annual Wellness Visit protocol.
If you or your family members are interested in learning how you can receive a cognitive assessment or dementia care from the comfort of home, you can schedule a free consultation with one of our care coordinators by clicking this link or calling (855) 255-5917.
About the Author
Ben Williams, MD, PhD is a leader in Synapticure’s cognitive practice. Prior to joining Synapticure, Dr. Williams worked as a neurologist for decades, specializing in treating people with Alzheimer’s and various forms of dementia both in general practice and at multiple ADRCs. He did his neurology residency training at UCSD under Dr. Robert Katzman, who was the doctor that identified Alzheimer disease as the primary cause of dementia in the elderly. Later Dr. Williams returned to Texas, where he worked with another early Alzheimer’s leader, Dr. Roger Rosenberg. Most recently, Dr. Williams worked at the new ADRC that was developed at Wake Forest Medical School. Dr. Williams has been board certified in Behavioral Neurology and Neuropsychology by UCNS since 2012.
Your first consultation with a care navigator is at no cost. Give us a call at 855-255-5917 for details.
